Few topics in women’s health are as commercially saturated, and as clinically misunderstood, as ovarian reserve testing. Over the past decade, direct-to-consumer companies have marketed AMH testing as a “biological clock test” or “egg timer”, promising women a clear answer to one of the most personal questions of their adult lives: how much time do I have?
The reality is more complicated, and considerably more nuanced, than the marketing suggests.
Both AMH and AFC are real, validated clinical tools, but they are tools designed to answer a very specific clinical question, and that question is not “when should I have children?” In this article, we examine what these markers actually measure, where their clinical value is genuine, where it breaks down, and what a more honest fertility assessment looks like.
What AMH and AFC actually measure
To understand the limits of these tests, it helps to understand what they are.
AMH (Antimüllerian Hormone) is a hormone secreted by the granulosa cells of small, growing follicles in the ovary. Specifically, it comes from preantral and small antral follicles (those under about 6 mm in diameter)1. Because these follicles are continuously being recruited from the resting primordial pool, the circulating level of AMH is roughly proportional to the size of that remaining pool2. AMH is gonadotropin-independent, which means its levels stay relatively stable across the menstrual cycle, making it convenient to test at any point3.
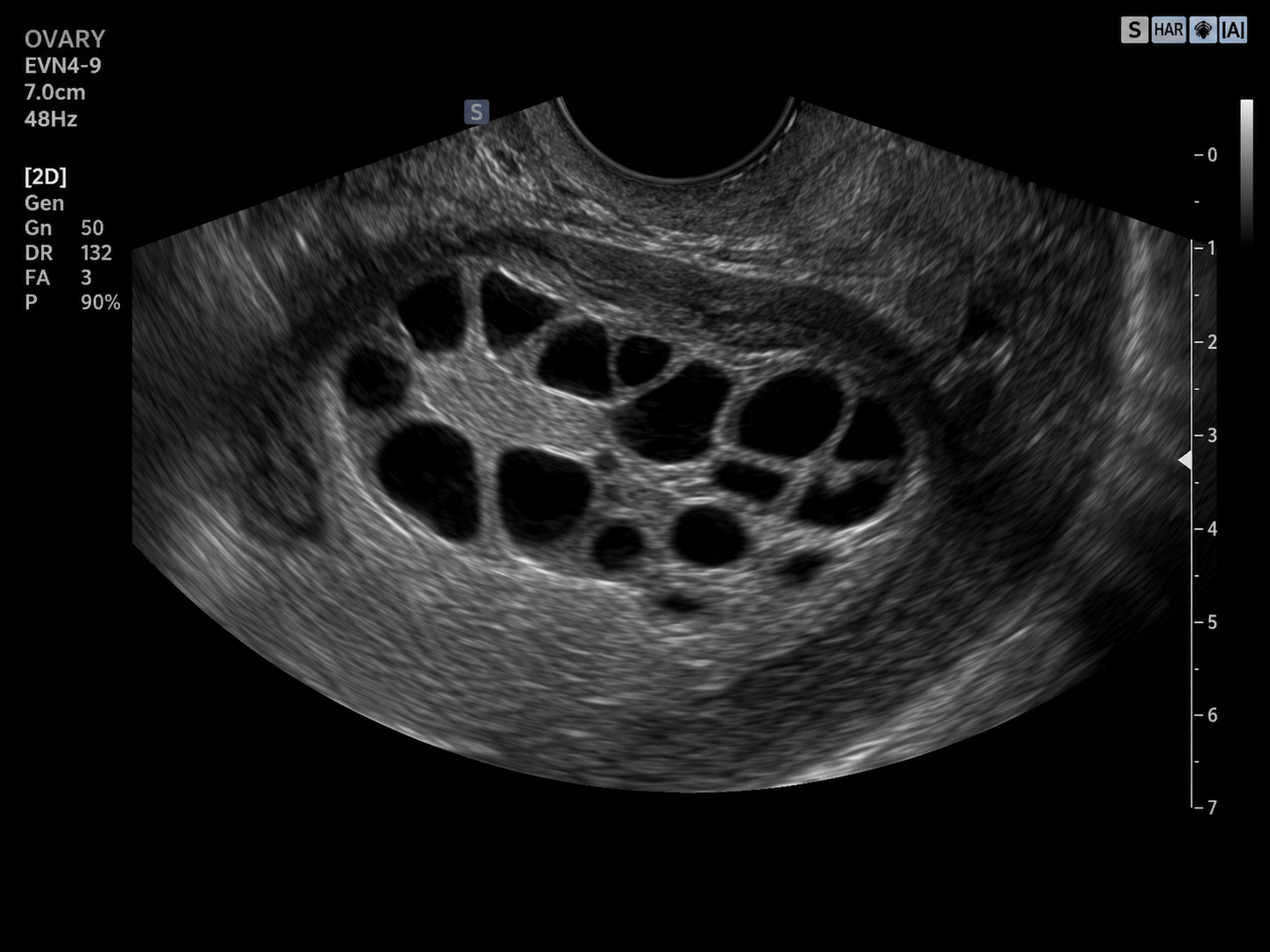
AFC (Antral Follicle Count) is the number of small fluid-filled follicles (2 to 10 mm in diameter) visible on a transvaginal ultrasound during the early follicular phase of the cycle, typically days 2 to 42. Because the follicles being counted on ultrasound are largely the same follicles producing AMH, the two markers correlate strongly with one another.
Together, AMH and AFC tell us approximately how many follicles are currently available for recruitment. They are estimators of the size of the pipeline, not of the quality of what comes through it.
Where AMH and AFC are genuinely useful
The clinical value of AMH and AFC is most pronounced in the context of assisted reproductive technology (ART), particularly IVF and egg freezing4.
In these settings, predicting the quantitative yield of oocytes is essential. It allows the reproductive endocrinologist to:
- Individualise the dose of gonadotropin medication
- Identify women at high risk of Ovarian Hyperstimulation Syndrome (OHSS) and adjust the protocol accordingly
- Recognise women likely to be poor responders and consider adjuvant strategies
- Set realistic expectations for the cycle
A systematic review of 28 studies showed that AMH has excellent discriminatory ability for predicting a poor ovarian response, with an Area Under the Curve (AUC) of 0.784. For predicting a high response, AMH performs even better. AMH also has superior analytical reproducibility compared to AFC, which depends heavily on the operator and the quality of the ultrasound equipment4.
In approximately 13 % of IVF patients, AMH and AFC results disagree with each other5. In those cases of discordance, large retrospective studies have shown that AFC is the more reliable predictor of how many eggs will actually be retrieved during a treatment cycle5. A woman with low AMH but a normal AFC of six or more still has a moderate-to-high likelihood of a normal response to ovarian stimulation5.
This is the clinical context in which these markers were originally validated, and it is the context in which they should be interpreted.
Where they fall short: predicting natural fertility
The mistake that has been embedded into direct-to-consumer fertility testing is the assumption that a marker which predicts IVF response must also predict natural fertility.
The evidence shows it does not, at least not on its own.
The most rigorous evidence on this question comes from large prospective trials of women without a history of infertility, attempting to conceive naturally.
The Time to Conceive study followed 750 women aged 30 to 44 with no known history of infertility, all of whom had been attempting to conceive for three months or less6. The investigators measured AMH and FSH at baseline and tracked cumulative pregnancy rates. The result: women with low AMH (below 0.7 ng/mL) and women with elevated early follicular FSH had cumulative pregnancy rates after six and twelve cycles that were statistically indistinguishable from those with normal markers6. A three-year follow-up of the same cohort confirmed that low AMH did not predict future infertility or compromised live birth rates7.
The EAGER (Effects of Aspirin in Gestation and Reproduction) trial evaluated 1,202 women aged 18 to 40 with a history of pregnancy loss. Women with low AMH levels (under 1.0 ng/mL) exhibited cumulative pregnancy rates that were comparable to those with normal AMH values7.
These findings have been reinforced by the 2025 editorial position of the journal Fertility and Sterility, which concluded plainly that AMH levels do not influence the time to spontaneous conception8.
Why? Because of one fundamental fact about reproductive biology.
The quantity-quality problem
Spontaneous conception is a qualitative event. It requires only a single, developmentally competent oocyte to be selected, ovulated, fertilised, and successfully implanted.
AMH and AFC measure the quantitative pool of available follicles. They do not measure, and cannot measure, whether those follicles will produce chromosomally normal eggs.
Egg quality is determined almost entirely by chronological age. At age 25, roughly 25 % of a woman’s eggs are chromosomally abnormal (aneuploid). By age 40, that figure rises to approximately 50 %. By age 42, it reaches 75 %9.
This produces two clinical scenarios that single-marker testing handles poorly:
- A 31-year-old with low AMH has low quantity but high quality. Her monthly chance of natural conception remains excellent because her age-associated egg quality is still good.
- A 41-year-old with high AMH has high quantity but low quality. She will respond impressively to IVF stimulation, but her natural monthly chance of pregnancy remains low because her age-related aneuploidy rate is the true limiting factor.
A high AMH does not protect against age-related decline in egg quality. A low AMH does not prevent natural conception. The two variables (quantity and quality) move on separate timelines and are determined by different biological processes.
The confounders that distort single readings
Even setting aside the quantity-quality problem, a single AMH or AFC reading can be misleading for biological reasons that have nothing to do with ovarian reserve.
Hormonal contraceptives suppress AMH. Combined oral contraceptive pills, hormonal rings, and other forms of hormonal birth control suppress the hypothalamic-pituitary-ovarian (HPO) axis and artificially lower measured AMH levels by approximately 19 % to 30 %10. A woman tested while on the pill, or in the months immediately after stopping, will see a falsely suppressed result.
Month-to-month variation is normal. Although AMH is far more stable than FSH or estradiol, AMH levels can naturally fluctuate by 20 % to 30 % from one month to the next, because a different cohort of follicles is recruited each cycle11. This means that repeated testing often shows “declines” or “improvements” that are simply normal biological noise.
Vitamin D deficiency can suppress AMH. Severe Vitamin D deficiency has been associated with artificially lower AMH readings, independent of true ovarian reserve.
PCOS can inflate AMH. Women with Polycystic Ovary Syndrome often have AMH levels two to three times higher than expected for their age, not because their fertility is superior, but because they have a larger pool of small antral follicles that fail to mature properly1.
A single reading interpreted out of context risks all of these confounders being mistaken for true clinical findings.
The menopause prediction problem
A common claim used to justify routine AMH testing is that the test can predict when a woman will reach menopause. This holds at a population level. At an individual level, it is far less precise than the claim suggests.
For women in their 20s and 30s, who are precisely the population for whom this prediction would be most clinically relevant, the confidence intervals for predicting the age of menopause from AMH range from 2 to 12 years of error12. An AMH test cannot reliably distinguish between a 31-year-old who will reach menopause at 43 and one who will reach it at 51.
The hypothesis that tracking AMH decline serially (rather than relying on a single measurement) might sharpen this prediction has also been tested and disproven. The Doetinchem Cohort Study, which tracked women over 20 years with serial AMH measurements, demonstrated that knowing an individual’s rate of AMH decline does not improve menopause prediction beyond a single baseline value12.
The exception is at the extremes. An AMH level below 0.2 ng/mL is associated with a median time to menopause of approximately six years, with around 60 % of women in this range undergoing menopause within five years7. An undetectable AMH (below 0.0018 ng/mL), interpreted alongside age and clinical symptoms, can predict the final menstrual period within 12 months7. These late-stage signals are useful, but they arrive far too close to menopause to provide any meaningful window for reproductive planning.
What actually tells us about the fertility window
If AMH and AFC cannot define a woman’s fertility window on their own, what rounds out the picture? Several factors add information that a hormone panel alone cannot.
1. Chronological age. Age remains the most accurate and powerful predictor of egg quality and ongoing fecundity. Because natural fertility typically ends approximately 5 to 10 years before menopause, and because average menopause occurs around 51, the practical end of natural fertility for most women falls in the mid-40s. Age sets the broad ceiling that the other markers operate within.
2. Family history. A mother’s age at natural menopause is a strong, clinically validated proxy for her daughter’s. A family history of early menopause (before age 45) or Premature Ovarian Insufficiency (before age 40) is a powerful signal that warrants early, proactive evaluation.
3. Menstrual cycle dynamics. A subtle, progressive shortening of the menstrual cycle (for example, a cycle that consistently drops from 28 days to 24 or 25 days) typically reflects an accelerated follicular phase caused by rising baseline FSH. The clinical onset of cycle shortening or cycle irregularity is a far more active, physiological indicator of a closing fertility window than any static lab value.
4. The full clinical picture. Reproductive success depends on far more than ovarian reserve. It requires normal ovulatory function, fallopian tube patency, a receptive uterine lining, healthy thyroid and metabolic function, and male partner factors (which are sole or contributing causes in approximately 50 % of all infertility cases)13. These variables sit outside what an AMH or AFC test can capture, which is exactly why they belong in the same assessment.
Why interpretation matters
When these markers are read in isolation, the consequences are not theoretical.
Misplaced anxiety. A young, healthy woman who receives a low AMH result may experience severe anxiety, conclude she is subfertile, and be funnelled toward expensive, invasive procedures such as elective oocyte cryopreservation, often without medical indication.
False reassurance. Conversely, a woman in her late 30s or early 40s with a high AMH may receive a false sense of security and delay childbearing, under the assumption that a high quantitative reserve protects her from age-related decline. It does not.
Commercial harm. A 2023 analysis of direct-to-consumer AMH testing websites found that three-quarters claimed AMH testing could predict overall fertility, three-quarters claimed it could predict the timing of menopause, and a similar proportion claimed it allowed women to adjust their reproductive timelines14. Given the evidence above, all three claims are misleading.
Where the experts land
There is genuine debate within reproductive medicine about how freely AMH should be offered, and the debate is instructive.
On one side, several major bodies have urged caution about testing women who are not seeking fertility care:
- The American College of Obstetricians and Gynecologists (ACOG) Committee Opinion No. 773 advises against routine AMH testing in women who are not currently seeking fertility care15.
- The American Society for Reproductive Medicine (ASRM) cautions against using ovarian reserve tests to predict natural fertility in non-infertile women16.
- The European Society of Human Reproduction and Embryology (ESHRE) takes a broadly similar position.
On the other side, clinicians such as Dr. Natalie Crawford argue (notably in her open letter “Dear ACOG, No”) that withholding this information is paternalistic, and that a single baseline AMH test, properly interpreted alongside age, family history, and full clinical context, can be a legitimate and empowering part of proactive reproductive planning17. The information itself is not the problem; the way it is presented and interpreted is.
What both sides actually agree on is the crucial distinction: between using AMH as one data point in a comprehensive assessment and using it as a standalone fertility score. The first is sound clinical medicine. The second is where things go wrong.
A clinically sound approach
A baseline fertility evaluation in a properly resourced clinical setting looks nothing like a direct-to-consumer AMH test.
At minimum, it involves:
- A cycle day 2 to 4 blood panel including AMH, FSH, estradiol, and LH, interpreted together (because elevated estradiol can artificially suppress FSH into the normal range, masking diminished ovarian reserve)
- A transvaginal ultrasound to perform an Antral Follicle Count and to assess uterine and ovarian structure (endometrial thickness, fibroids, polyps, cysts)
- A thorough history, including menstrual cycle pattern, family history of menopause and reproductive health, and lifestyle factors
- An assessment of thyroid function, metabolic health, and Vitamin D, all of which influence fertility through pathways unrelated to ovarian reserve
- For women in partnerships, a male partner evaluation, because approximately half of all infertility cases involve male factors
This is what comprehensive ovarian reserve assessment actually looks like. A single number, sold online and interpreted in isolation, is not.
To wrap it up: what does all this mean?
AMH and AFC are valuable clinical tools. In the right context (predicting response to ovarian stimulation in IVF and egg freezing) they are among the best biomarkers reproductive medicine has.
But read in isolation, as standalone fertility scores, they tell only part of the story. On their own they cannot separate quantity from quality, they cannot account for the dominant role of chronological age, and they can be distorted by common confounders such as hormonal contraception. Interpreted alongside the wider clinical picture, those same numbers become genuinely informative.
The honest clinical answer to the question “how much time do I have?” is not contained in a single hormone test. It lies in the integration of age, family history, cycle dynamics, structural health, metabolic and thyroid function, partner factors, and yes, where appropriate, a properly interpreted AMH and AFC.
Fertility planning is too important to be reduced to a single marker. Women deserve the full picture.